Understanding Severe Microcephaly: Clinical Implications of a 14 cm Head Circumference
The birth of a child brings a flood of medical assessments designed to ensure the health and stability of the newborn. One of the primary measurements taken immediately after delivery is the occipitofrontal circumference (OFC), commonly known as head circumference. While small variations in size are normal, a measurement of 14 cm in a newborn is a significant clinical finding that requires immediate neurological and neonatal investigation.
Defining the Measurement: The Significance of 14 cm
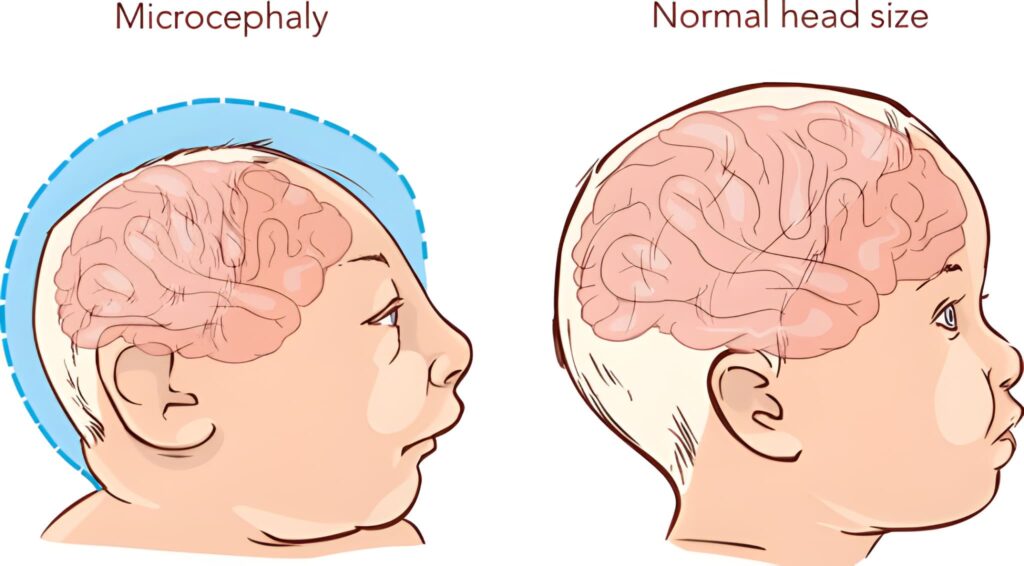
To understand the gravity of a 14 cm head circumference, one must first look at the standard benchmarks for a full-term infant. A typical newborn, born between 37 and 42 weeks of gestation, usually presents with a head circumference ranging from 33 cm to 35 cm. A measurement of 14 cm falls more than three standard deviations below the mean, placing it in the category of severe microcephaly.
When a head circumference is this small, it indicates that the brain has either not developed correctly during pregnancy or has stopped growing at an early stage of gestation. The skull grows in response to the pressure of the expanding brain; therefore, a significantly small skull is almost always a reflection of an underlying brain development issue.
Clinical Implications: What This Means for the Newborn
A 14 cm head circumference is often associated with severe neurological impairment. The brain structures responsible for basic life functions, such as breathing, heart rate regulation, and swallowing, may be affected. In many cases, this measurement is seen in infants born at the very edge of viability (extremely preterm) or in full-term infants with profound developmental anomalies.
Potential for severe cognitive delays, motor function impairments, and seizures as the electrical activity of the brain may be disorganized.
Increased risk of respiratory distress, feeding difficulties, and challenges with temperature regulation due to an underdeveloped central nervous system.
Potential Causes & Etiology
Medical professionals categorize the causes of severe microcephaly into two primary groups: primary (genetic or developmental) and secondary (environmental or disruptive). Determining the cause is vital for both the immediate care of the infant and for providing the family with information regarding future pregnancies.
| Category | Potential Causes | Description |
|---|---|---|
| Genetic Anomalies | Chromosomal Disorders | Conditions like Trisomy 13 or Trisomy 18 often present with severe microcephaly. |
| In-Utero Infections | TORCH Infections | Zika virus, Cytomegalovirus (CMV), and Toxoplasmosis can halt brain growth. |
| Cerebral Insults | Hypoxic-Ischemic Events | A severe lack of blood flow or oxygen to the brain early in pregnancy. |
| Structural Defects | Anencephaly/Encephalocele | Neural tube defects where portions of the brain or skull fail to form. |
The Diagnostic Process: Next Steps in the Hospital
Once the initial measurement is confirmed, the neonatal team initiates a series of diagnostic tests to understand the brain's internal structure and function. This process typically involves a multidisciplinary team, including neonatologists, pediatric neurologists, and geneticists.
The team usually performs a cranial ultrasound first as it is non-invasive and can be done at the bedside. However, for a 14 cm measurement, an MRI or CT scan provides the detailed imagery necessary to identify missing structures, calcifications, or malformations of the cortex.
Chromosomal microarray or whole-exome sequencing may be recommended. These tests look for tiny deletions or duplications in the DNA that could explain why the brain did not develop to its expected size.
An Electroencephalogram (EEG) measures the brain's electrical activity. This is crucial for detecting subclinical seizures, which are common in infants with severe brain development issues.
NICU Management & Palliative Care
In the Neonatal Intensive Care Unit (NICU), the primary goal for an infant with a 14 cm head circumference is stability and comfort. The medical team focuses on maintaining the baby’s airway, ensuring hydration, and managing any pain or discomfort.
Respiratory Support: Depending on the baby's ability to drive their own breathing, the team may use various levels of support, from simple nasal cannulas to mechanical ventilation. However, if the brain stem is severely affected, the infant may not be able to sustain independent respiration.
Feeding and Nutrition: Many infants with severe microcephaly struggle with the "suck-swallow-breathe" coordination. In these cases, a nasogastric (NG) tube may be used to provide nutrition directly to the stomach.
Support for Families and Caregivers
Receiving news of a critical measurement like 14 cm is a traumatic event for parents. The emotional toll of navigating a complex medical diagnosis while also recovering from childbirth is immense. Hospitals provide social workers, chaplains, and bereavement counselors to help families process the information and make difficult decisions.
It is essential for parents to ask questions and seek clarity from the medical team. Understanding the short-term and long-term prognosis helps in making informed decisions about interventions and care goals. Families should also be encouraged to reach out to specialized support organizations that focus on microcephaly and rare neurological conditions.
Questions to Ask Your Medical Team
- What do the imaging results show regarding the internal structures of the brain?
- Is the baby experiencing any seizure activity?
- Are the basic life-sustaining reflexes (breathing, swallowing) present?
- What is the recommended level of intervention based on the current findings?
- Can we meet with a genetic counselor to discuss the findings?
While the clinical reality of a 14 cm head circumference is daunting, the medical community remains dedicated to providing the highest level of care for the infant and comprehensive support for the family during this challenging time.



